")
")
Angioplasty

Coronary Artery Angioplasty
Coronary angioplasty is a non-surgical procedure to open (widen) narrowed or blocked coronary arteries. It is done using the same technique as coronary angiography. Coronary angioplasty can be performed by simply opening the narrowed coronary artery with a balloon or accompanied by placement of an intracoronary metallic prosthesis (stent).
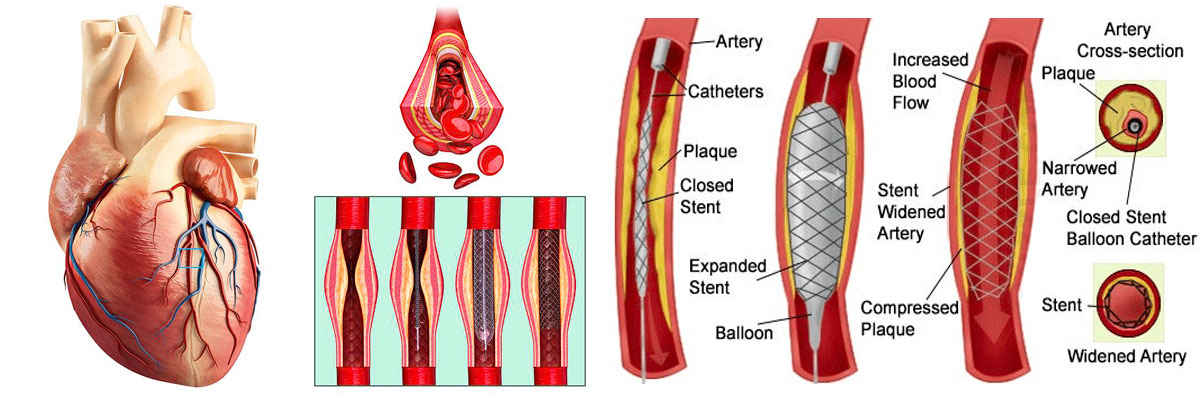
Balloon Angioplasty
In this procedure a small catheter with a balloon tip is used to open the blocked coronary artery. The operation usually takes less than an hour and patients leave the hospital the next day. The first part of balloon angioplasty is similar to that of cardiac catheterization (preparation, insertion of catheters, and injection of contrast medium). Then with the help of X-rays, the doctor advances a small metal wire through the narrowed coronary artery. A balloon is advanced with the help of the wire and placed at the site of the narrowing. The balloon is expanded (inflated) thus compressing the atherosclerotic plaque against the artery wall. The balloon stays inflated for several seconds before deflating. With the help of X-rays, the doctor checks the effect of the expansion. If the lumen of the coronary artery at the site of the stenosis has been sufficiently opened and a smooth flow of blood to the heart is ensured, the balloon is removed and the operation is complete.
Angioplasty with placement of a metal prosthesis (stent)
A stent is a small metal tube with gaps that is placed at the site of the narrowing of the coronary artery, after it has been previously opened with a balloon, to keep the artery open. The metal prosthesis is placed on a balloon catheter and with the help of X-rays is positioned at the site of the narrowing of the coronary artery. The balloon is inflated thus leading to the opening of the metal prosthesis that stays in contact with the artery wall. One or more metal prostheses may be used depending on the length of the narrowing. An X-ray check is done to assess the effect of the opening and placement of the metal prosthesis. The balloon can be re-expanded several times until we ensure that the metal prosthesis is properly positioned and stretched at the site of the stenosis. After a satisfactory result is achieved, the balloon is deflated and withdrawn along the wire from the point of constriction. The metal prosthesis remains at the site of the narrowing, keeping the artery open. After the procedure, the catheter entry point is closed with the help of various substances (collagen) or sutures in large vessels (femoral artery). In some cases, the small tube (catheter) can remain in the artery of the groin and be removed a few hours later when the coagulative state of the body allows it, applying pressure to this point with the hands. For the closure of radial artery puncture site external pressure is applied by means of a special bracelet, which is gradually loosened and after few hours withdrawn.
Angioplasty of the peripheral vessels
Peripheral angioplasty refers to the use of a balloon to open a blood vessel anywhere in the body other than the coronary arteries. It is most commonly used to treat atherosclerotic narrowing of the abdominal, leg, and renal arteries caused by peripheral arterial disease.
Carotid angioplasty
Carotid artery stenosis can be treated with stent angioplasty for patients who might otherwise undergo carotid endarterectomy (CEA). Although carotid endarterectomy is preferred over stent angioplasty, this option is contraindicated in selected patients who have serious health problems, such as medical comorbidities (coronary heart disease, heart failure, chronic obstructive pulmonary disease) and anatomical features (contralateral internal carotid occlusion, radiation therapy in the neck, previous carotid surgery, intrathoracic or intracranial carotid disease) that would make surgery difficult and dangerous.
Angioplasty of the veins
Angioplasty is used to treat venous stenosis, which affects dialysis. Drug-infusion angioplasty proves to have better patency than conventional balloon angioplasty at 6 and 12 months after surgery. Angioplasty is also occasionally used to treat residual subclavian vein stenosis after thoracic outlet surgical decompression in thoracic outlet syndrome. Finally, stent angioplasty is recommended for the treatment of occlusion in chronic venous disease.
Why is stent angioplasty usually preferred?
Stent angioplasty is preferred for:
- Preventing re-narrowing of the artery.
- Preventing detachment of small pieces of atherosclerotic plaque.
- The sealing of any openings in the walls of the artery.
Are there complications with angioplasty?
Complications of angioplasty are rare. In less than 1% of patients undergoing angioplasty, emergency coronary artery bypass grafting may be required, and operative mortality in specialized centers is less than 0.5%. In an also very small percentage (1-2%), blockage of the coronary artery thrombus may occur at the point of placement of the intracoronary prosthesis (stent) in the following hours after the operation or even in the following days after leaving the Hospital. This occlusion is usually reopened in the Catheterization Laboratory and rarely requires coronary artery bypass surgery. The risk of myocardial infarction after angioplasty is 2-5%, resulting from sidebranch occlusion occurring after stenting, embolization of material from the stenosis to the periphery of the vessel, or thrombosis of the stent.